
The Human Factors Analysis and Classification System—HFACS Cover
and Documentation
Introduction
1. Unsafe Acts
2. Preconditions
for Unsafe Acts
3. Unsafe Supervision
4. Organizational
Influences
Conclusion
References
HFACS and Wildland Fatality Investigations
Hugh Carson wrote this
article a few days after the Cramer Fire
Bill Gabbert wrote this article following the release of the Yarnell Hill Fire ADOSH report
A Roadmap to a Just Culture:
Enhancing the Safety Environment
Cover
and Contents
Forward by James Reason
Executive Summary
1. Introduction
2. Definitions and Principles of a Just Culture
3. Creating a Just Culture
4. Case Studies
5. References
Appendix A. Reporting Systems
Appendix B. Constraints to a Just Reporting Culture
Appendix C. Different Perspectives
Appendix D. Glossary of Acronyms
Appendix E. Report Feedback Form
Rainbow Springs Fire, 1984 — Incident Commander Narration
Introduction
Years Prior
April 25th
Fire Narrative
Lessons Learned
Conclusion
Tools to Identify Lessons Learned
An FAA website presents 3
tools to identify lessons learned from accidents. The site also
includes an animated
illustration of a slightly different 'Swiss-cheese' model called "defenses-in-depth."
|
The Human Factors Analysis and Classification System–HFACS
The “Swiss cheese” model
of accident causation
February 2000
Introduction
Sadly, the annals of aviation history are littered with accidents and
tragic losses. Since the late 1950s, however, the drive to reduce the
accident rate has yielded unprecedented levels of safety to a point where
it is now safer to fly in a commercial airliner than to drive a car or
even walk across a busy New York city street. Still, while the aviation
accident rate has declined tremendously since the first flights nearly
a century ago, the cost of aviation accidents in both lives and dollars
has steadily risen. As a result, the effort to reduce the accident rate
still further has taken on new meaning within both military and civilian
aviation.
Even with all the innovations and improvements realized in the last
several decades, one fundamental question remains generally unanswered:
“Why do aircraft crash?” The answer may not be as straightforward
as one might think. In the early years of aviation, it could reasonably
be said that, more often than not, the aircraft killed the pilot. That
is, the aircraft were intrinsically unforgiving and, relative to their
modern counterparts, mechanically unsafe. However, the modern era of aviation
has witnessed an ironic reversal of sorts. It now appears to some that
the aircrew themselves are more deadly than the aircraft they fly (Mason,
1993; cited in Murray, 1997). In fact, estimates in the literature indicate
that between 70 and 80 percent of aviation accidents can be attributed,
at least in part, to human error (Shappell & Wiegmann, 1996). Still,
to off-handedly attribute accidents solely to aircrew error is like telling
patients they are simply “sick” without examining the underlying
causes or further defining the illness.
So what really constitutes that 70-80 % of human error repeatedly referred
to in the literature? Some would have us believe that human error and
“pilot” error are synonymous. Yet, simply writing off aviation
accidents merely to pilot error is an overly simplistic, if not naive,
approach to accident causation. After all, it is well established that
accidents cannot be attributed to a single cause, or in most instances,
even a single individual (Heinrich, Petersen, and Roos, 1980). In fact,
even the identification of a “primary” cause is fraught with
problems. Rather, aviation accidents are the end result of a number of
causes, only the last of which are the unsafe acts of the aircrew (Reason,
1990; Shappell & Wiegmann, 1997a; Heinrich, Peterson, & Roos,
1980; Bird, 1974).
The challenge for accident investigators and analysts alike is how best
to identify and mitigate the causal sequence of events, in particular
that 70-80 % associated with human error. Armed with this challenge, those
interested in accident causation are left with a growing list of investigative
schemes to chose from. In fact, there are nearly as many approaches to
accident causation as there are those involved in the process (Senders
& Moray, 1991). Nevertheless, a comprehensive framework for identifying
and analyzing human error continues to elude safety professionals and
theorists alike. Consequently, interventions cannot be accurately targeted
at specific human causal factors nor can their effectiveness be objectively
measured and assessed. Instead, safety professionals are left with the
status quo. That is, they are left with interest/fad-driven research resulting
in intervention strategies that peck around the edges of accident causation,
but do little to reduce the overall accident rate. What is needed is a
framework around which a needs-based, data-driven safety program can be
developed (Wiegmann & Shappell, 1997).
Reason’s “Swiss Cheese” Model of Human Error
One particularly appealing approach to the genesis of human error is
the one proposed by James Reason (1990). Generally referred to as the
“Swiss cheese” model of human error, Reason describes four
levels of human failure, each influencing the next (Figure 1). Working
backwards in time from the accident, the first level depicts those Unsafe
Acts of Operators that ultimately led to the accident[1].
More commonly referred to in aviation as aircrew/pilot error, this level
is where most accident investigations have focused their efforts and consequently,
where most causal factors are uncovered. After all, it is typically the
actions or inactions of aircrew that are directly linked to the accident.
For instance, failing to properly scan the aircraft’s instruments
while in instrument meteorological conditions (IMC) or penetrating IMC
when authorized only for visual meteorological conditions (VMC) may yield
relatively immediate, and potentially grave, consequences. Represented
as “holes” in the cheese, these active failures are typically
the last unsafe acts committed by aircrew.
[1] Reason’s original work involved operators
of a nuclear power plant. However, for the purposes of this manuscript,
the operators here refer to aircrew, maintainers, supervisors and
other humans involved in aviation.
However, what makes the “Swiss cheese” model particularly
useful in accident investigation, is that it forces investigators to address
latent failures within the causal sequence of events as well. As their
name suggests, latent failures, unlike their active counterparts, may
lie dormant or undetected for hours, days, weeks, or even longer, until
one day they adversely affect the unsuspecting aircrew. Consequently,
they may be overlooked by investigators with even the best intentions.
Within this concept of latent failures, Reason described
three more levels of human failure. The first involves the condition of
the aircrew as it affects performance. Referred to as Preconditions
for Unsafe Acts, this level involves conditions such as mental fatigue
and poor communication and coordination practices, often referred to as
crew resource management (CRM). Not surprising, if fatigued aircrew fail
to communicate and coordinate their activities with others in the cockpit
or individuals external to the aircraft (e.g., air traffic control, maintenance,
etc.), poor decisions are made and errors often result.
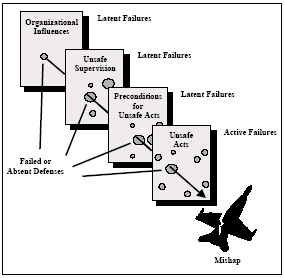
Figure 1. The “Swiss cheese” model of human error causation
(adapted from Reason, 1990).
But exactly why did communication and coordination break down in the
first place? This is perhaps where Reason’s work departed from more
traditional approaches to human error. In many instances, the breakdown
in good CRM practices can be traced back to instances of Unsafe Supervision,
the third level of human failure. If, for example, two inexperienced (and
perhaps even below average pilots) are paired with each other and sent
on a flight into known adverse weather at night, is anyone really surprised
by a tragic outcome? To make matters worse, if this questionable manning
practice is coupled with the lack of quality CRM training, the potential
for miscommunication and ultimately, aircrew errors, is magnified. In
a sense then, the crew was “set up” for failure as crew coordination
and ultimately performance would be compromised. This is not to lessen
the role played by the aircrew, only that intervention and mitigation
strategies might lie higher within the system.
Reason’s model didn’t stop at the supervisory level either;
the organization itself can impact performance at all levels. For instance,
in times of fiscal austerity, funding is often cut, and as a result, training
and flight time are curtailed. Consequently, supervisors are often left
with no alternative but to task “non-proficient” aviators
with complex tasks. Not surprisingly then, in the absence of good CRM
training, communication and coordination failures will begin to appear
as will a myriad of other preconditions, all of which will affect performance
and elicit aircrew errors. Therefore, it makes sense that, if the accident
rate is going to be reduced beyond current levels, investigators and analysts
alike must examine the accident sequence in its entirety and expand it
beyond the cockpit. Ultimately, causal factors at all levels within the
organization must be addressed if any accident investigation and prevention
system is going to succeed.
In many ways, Reason’s “Swiss cheese” model of accident
causation has revolutionized common views of accident causation. Unfortunately,
however, it is simply a theory with few details on how to apply it in
a real-world setting. In other words, the theory never defines what the
“holes in the cheese” really are, at least within the context
of everyday operations. Ultimately, one needs to know what these system
failures or “holes” are, so that they can be identified during
accident investigations or better yet, detected and corrected before an
accident occurs.
The balance of this paper will attempt to describe the “holes in
the cheese.” However, rather than attempt to define the holes using
esoteric theories with little or no practical applicability, the original
framework (called the Taxonomy of Unsafe Operations) was developed
using over 300 Naval aviation accidents obtained from the U.S. Naval Safety
Center (Shappell & Wiegmann, 1997a). The original taxonomy has since
been refined using input and data from other military (U.S. Army Safety
Center and the U.S. Air Force Safety Center) and civilian organizations
(National Transportation Safety Board and the Federal Aviation Administration).
The result was the development of the Human Factors Analysis and Classification
System (HFACS).
<<< continue
reading HFACS, Unsafe Acts >>>
|
